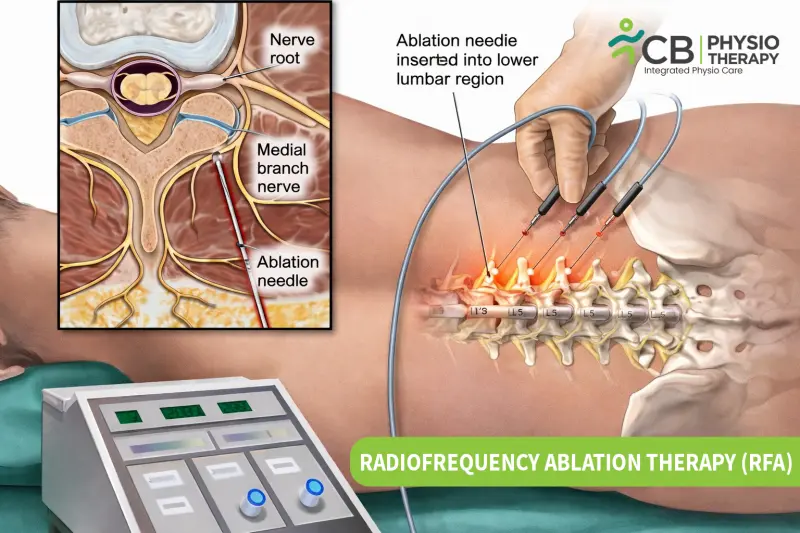
Radiofrequency Ablation (RFA) is a minimally invasive medical procedure that uses controlled radiofrequency energy (heat) to target specific pain-transmitting nerves. By reducing the nerve’s ability to send pain signals, RFA can provide meaningful relief and improve functional activity—often without the need for major surgery.
RFA is typically performed under fluoroscopy (C-Arm) or ultrasound guidance for precision and safety.
RFA is classified based on how energy is delivered and the effect on nerve/tissue:
1) Continuous RFA (Conventional)
-
Continuous high-frequency current
-
Controlled thermal lesioning (typically 60–90°C)
-
Used for longer-lasting pain relief (e.g., facet joint pain)
Goal: Neurodestruction to stop pain signals
2) Pulsed Radiofrequency (PRF)
-
Energy delivered in short bursts
-
Temperature kept below ~42°C
-
Does not destroy the nerve; modifies signaling
Goal: Neuromodulation (pain control without nerve damage)
3) Cooled Radiofrequency Ablation
-
Internally cooled probe tip
-
Creates a larger lesion zone for broader pain generators
Goal: Treat larger pain-generating areas with precision
4) Bipolar Radiofrequency Ablation
-
Uses two active electrodes
-
Produces focused lesions between electrodes
Goal: Higher precision in selected cases
The technique is chosen based on the diagnosis, target anatomy, and clinical goals.
RFA is used when pain arises from a clearly identifiable source and is often considered after diagnostic blocks confirm the pain generator.
Spine & Joint Pain
-
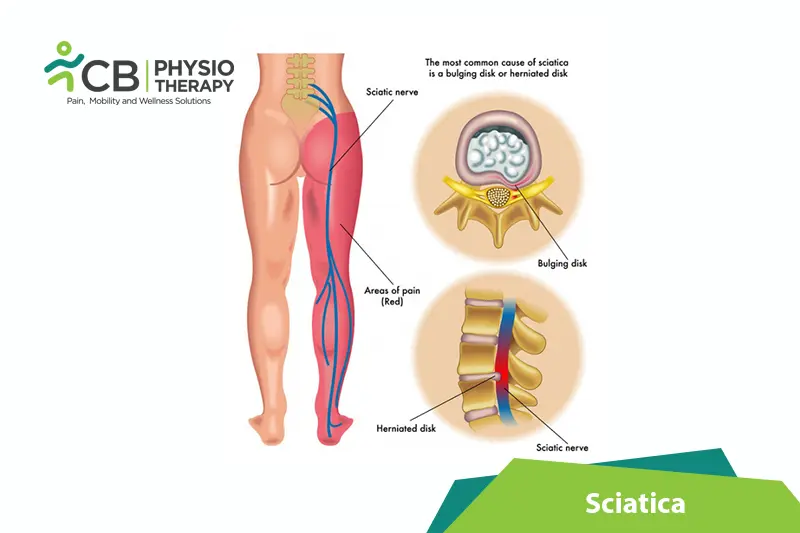
Lumbar facet joint pain (chronic low back pain)
-
Cervical facet pain (neck pain)
-
Sacroiliac joint pain
-
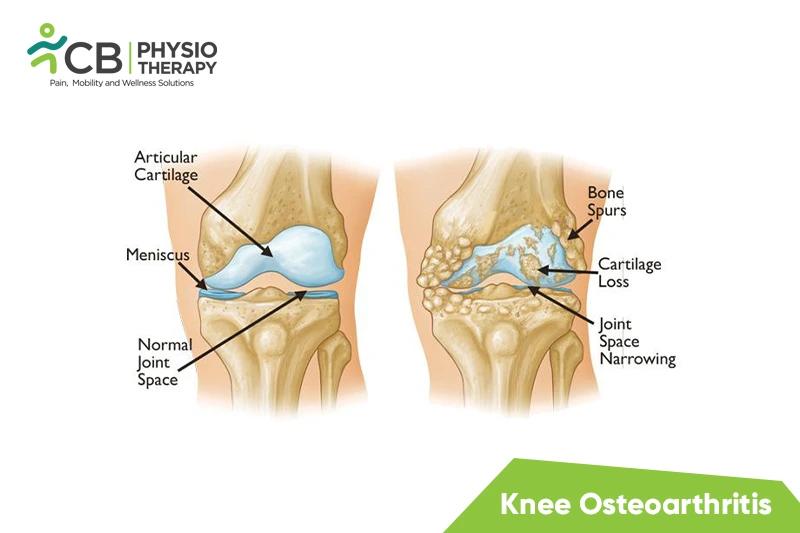
Knee osteoarthritis pain (genicular nerve RFA)
-
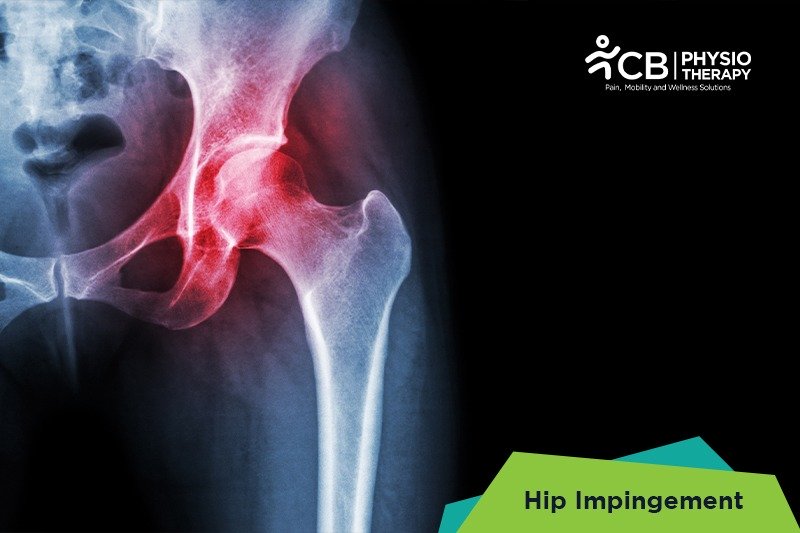
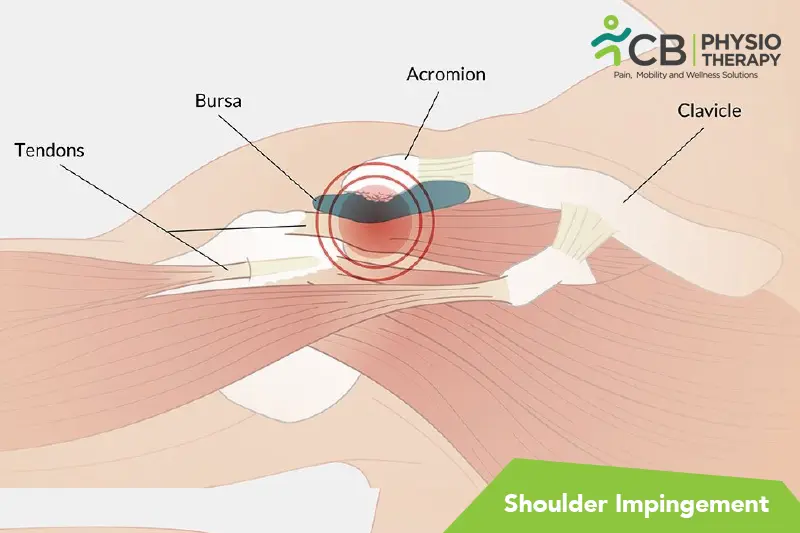
shoulder and hip joint pain
Nerve-Related Pain
-
Trigeminal neuralgia (selected cases)
-
Occipital neuralgia
-
Intercostal neuralgia
-
Post-surgical nerve pain
Selected Pelvic & Plexus Pain
-
Hypogastric plexus pain syndromes (selected cases)
During the procedure:
-
The skin is numbed using local anesthetic
-
A thin needle/probe is placed near the target nerve under imaging guidance
-
Sensory/motor testing may be performed to confirm safe positioning
-
Controlled radiofrequency energy is delivered to reduce pain signaling
Procedure time: typically 30–60 minutes
Stay: usually day-care, go home the same day
Relief onset: often gradual over days to weeks
Primary Physiological Effect
-
Interrupts pain-carrying nerve signals
Protein denaturation
Neuromodulation (in pulsed RFA)
Clinical Effects (What patients feel)
-
Reduced chronic pain
-
Improved mobility and joint tolerance
-
Decreased muscle guarding/spasm
-
Better ability to move, exercise, and rehabilitate
-
Improved comfort in daily activities
Secondary Rehabilitation Benefits
Once pain reduces:
-
Movement confidence improves
-
Physiotherapy becomes easier and more effective
-
Strength and functional capacity improve
Expected Temporary Local Effects
-
Mild soreness at the procedure site
-
Local swelling
-
Temporary numbness/tingling (in some cases)
Radiofrequency Ablation (RFA) offers a targeted, minimally invasive approach to managing chronic pain, helping patients achieve meaningful relief with less disruption to their daily lives.
-
Non-surgical pain relief: RFA addresses pain at its source without requiring major incisions or open surgery.
-
Minimally invasive procedure: Only a thin probe is inserted through the skin, resulting in minimal tissue disruption.
-
Longer-lasting relief: Many patients experience sustained pain reduction for months, sometimes longer, depending on the condition treated.
-
Faster recovery: Most individuals return to routine activities within 24–72 hours after the procedure.
-
Reduced medication dependence: Effective pain control may decrease reliance on long-term pain medications.
-
Improved mobility and function: As pain decreases, movement tolerance and participation in rehabilitation improve.
-
Repeatable when necessary: If nerves regenerate and pain returns, the procedure can often be safely repeated.
-
High precision: Imaging guidance allows accurate targeting of pain-transmitting nerves, enhancing both safety and effectiveness.
When performed by trained specialists under strict sterile technique and image guidance, RFA is considered a safe and well-established procedure for chronic pain.
Common short-term effects:
-
Mild soreness
-
Local swelling
-
Temporary numbness/tingling
Serious complications are uncommon in properly selected patients.
Relief can last 6–18 months, sometimes longer, depending on:
-
The condition treated
-
The nerve targeted
-
Individual healing and nerve regeneration
Since nerves can regenerate, RFA may be repeated if pain returns and it’s clinically appropriate.
You may be suitable if:
-
Pain has persisted > 3–6 months
-
Conservative treatment (physiotherapy/medications) has not helped enough
-
The pain source is confirmed—often via diagnostic nerve blocks
-
Surgery is not indicated or you prefer a non-surgical route
A detailed clinical evaluation is essential before recommending RFA.
Absolute Contraindications
-
Active local or systemic infection
-
Uncontrolled bleeding disorder
-
Unclear/uncertain pain diagnosis without confirmed pain source
-
Inability to safely position or cooperate during the procedure
Relative Contraindications (Require Caution/Optimization)
-
Blood thinners (anticoagulants)
-
Pregnancy (depends on target region and imaging needs)
-
Uncontrolled diabetes or hypertension
-
Implanted electrical devices (special precautions required)
In most cases:
-
1 session per target nerve/region is sufficient
Additional sessions may be needed if:
-
Multiple pain areas are treated (often staged)
-
Pain returns after months/years due to nerve regeneration
-
Partial response after the first session (selected cases)
Most patients report it is more comfortable than expected:
During preparation
-
Small pinch/sting from local anesthetic
During the procedure
-
Mild pressure
-
Brief warmth/buzzing sensation
-
Occasional dull ache or twitching
After the procedure
-
Mild soreness like a bruise
-
Temporary stiffness
-
Usually settles in a few days
Most people return to routine activity within 24–72 hours (as advised).
RFA and physiotherapy are not competing treatments—they are complementary.
-
RFA reduces the pain barrier
-
Physiotherapy restores movement, strength, and biomechanics
With structured physiotherapy after RFA:
-
Strength improves
-
Movement patterns normalize
-
Recurrence risk reduces
-
Long-term functional outcomes improve
This integration is often what turns pain relief into sustainable recovery.